Slide 1 of 20
Slide 1 - CGM in Obesity: Fact, Fad, or Future Tool?
A Rational Clinical Framework for Endocrinologists
Targeted Guidance for Obesity Medicine Specialists
---
Photo by Gabriella Clare Marino on Unsplash
Generated from prompt:
Redesign and modernize a physician-level presentation titled 'CGM in Obesity: Fact, Fad, or Future Tool? A Rational Clinical Framework for Endocrinologists.' Target audience: endocrinologists and obesity medicine specialists. Style: clean academic grand rounds, high visual hierarchy, minimal text per slide, strong clinical positioning. Structure (~35 slides): 1. Title slide (clean, modern) 2. Executive thesis: CGM selective utility, not routine therapy 3. Why this question matters (obesity vs diabetes burden) 4. Market expansion vs evidence timeline 5. Is obesity a glycemic disease? conceptual model 6. What CGM measures vs does not measure (visual comparison) 7. Postprandial physiology curves (lean vs obese vs T2DM) 8. Glycemic variability vs energy balance schematic 9. Personalized responses (Zeevi study concept) 10. Missing RCT problem 11. Evidence pyramid slide 12. RCT evidence summary (2020–2024) 13. CGM + coaching vs coaching alone 14. Observational attrition funnel 15. Metabolic outcomes independent of weight 16. Where CGM may help: Prediabetes phenotype 17. NAFLD & PCOS hypothesis slide 18. Behavioral neuroendocrinology model 19. Psychological risks 20. Physiologic misinterpretation risks 21. Cost-effectiveness comparison (dietitian, GLP-1, bariatric) 22. Commercial incentives slide 23. When CGM is rational (clinical criteria) 24. When NOT recommended 25. 14-day protocol overview 26–30. Protocol experiment slides (baseline, protein-first, walking, portion, consolidation) 31. Indian meal example clinical application 32. Future research priorities 33. Ideal RCT design summary 34. Fact vs Fad vs Future table 35. Take-home messages for endocrinologists Design instructions: white background, deep blue + teal accents, clean typography, bold headers, minimal bullets (max 5 per slide), diagrams instead of paragraphs where possible, executive clarity.
A rational clinical framework for endocrinologists on using Continuous Glucose Monitors (CGM) in obesity management. Covers obesity burden, CGM fundamentals, RCT evidence (2020-2024), rational indications, 14-day protocol, clinical examples, and未来研究.
A Rational Clinical Framework for Endocrinologists
Targeted Guidance for Obesity Medicine Specialists
---
Photo by Gabriella Clare Marino on Unsplash
---
Photo by Nathan Jeon on Unsplash
1
Navigating Hype in Obesity Management
---
Photo by Logan Voss on Unsplash
Source: Wikipedia: Obesity
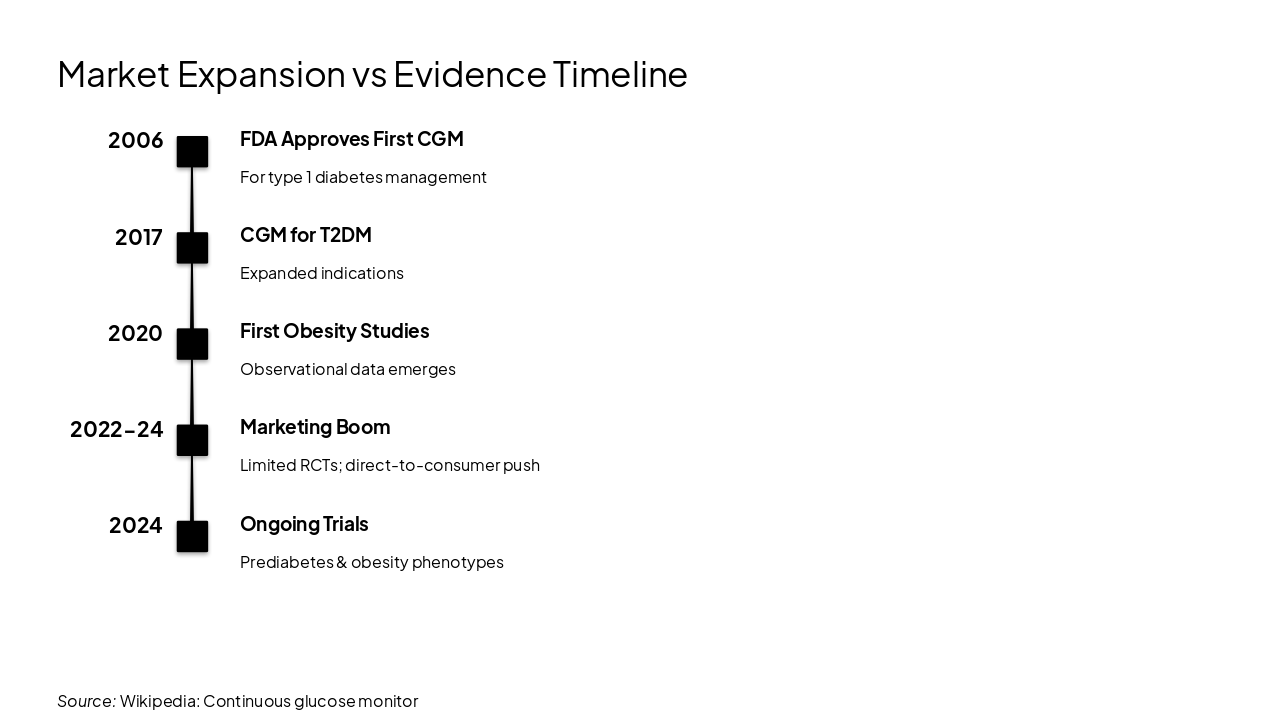
2006: FDA Approves First CGM For type 1 diabetes management 2017: CGM for T2DM Expanded indications 2020: First Obesity Studies Observational data emerges 2022-24: Marketing Boom Limited RCTs; direct-to-consumer push 2024: Ongoing Trials Prediabetes & obesity phenotypes
Source: Wikipedia: Continuous glucose monitor
2
Conceptual Model & Measurement Realities
---
Photo by Sweet Life on Unsplash
---
Photo by Sweet Life on Unsplash
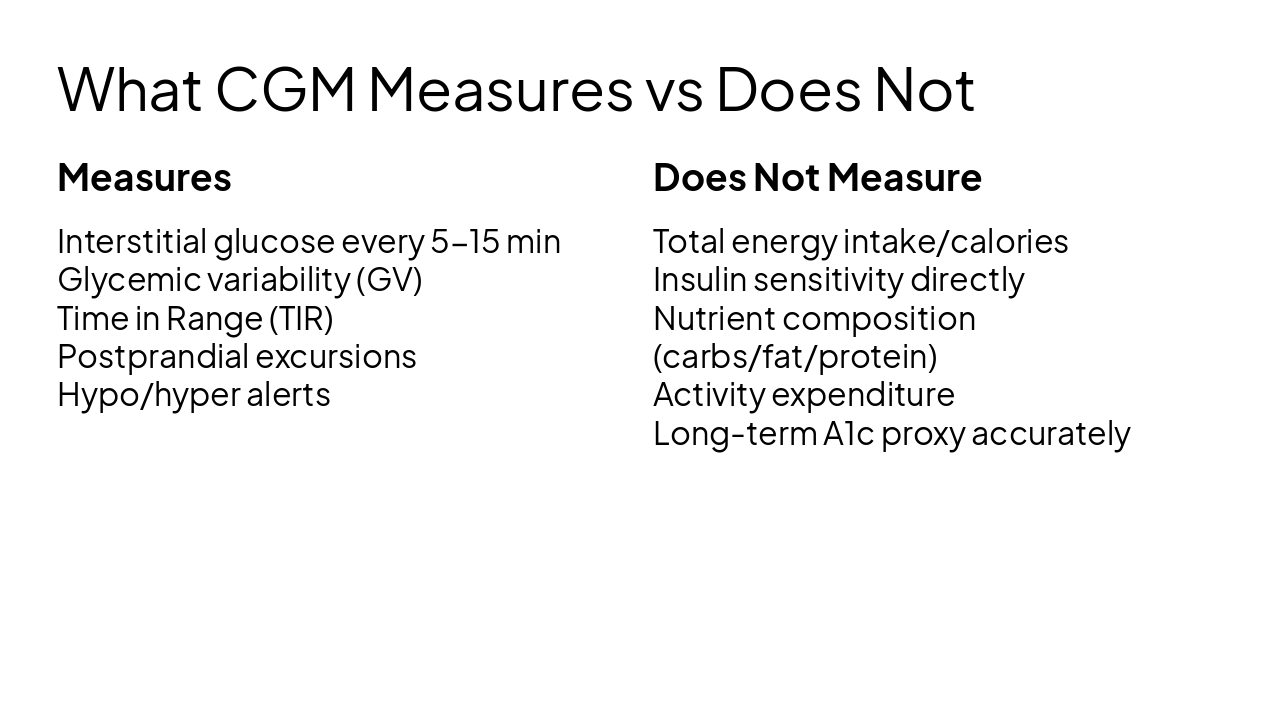
Measures Interstitial glucose every 5-15 min Glycemic variability (GV) Time in Range (TIR) Postprandial excursions Hypo/hyper alerts
Does Not Measure Total energy intake/calories Insulin sensitivity directly Nutrient composition (carbs/fat/protein) Activity expenditure Long-term A1c proxy accurately
3
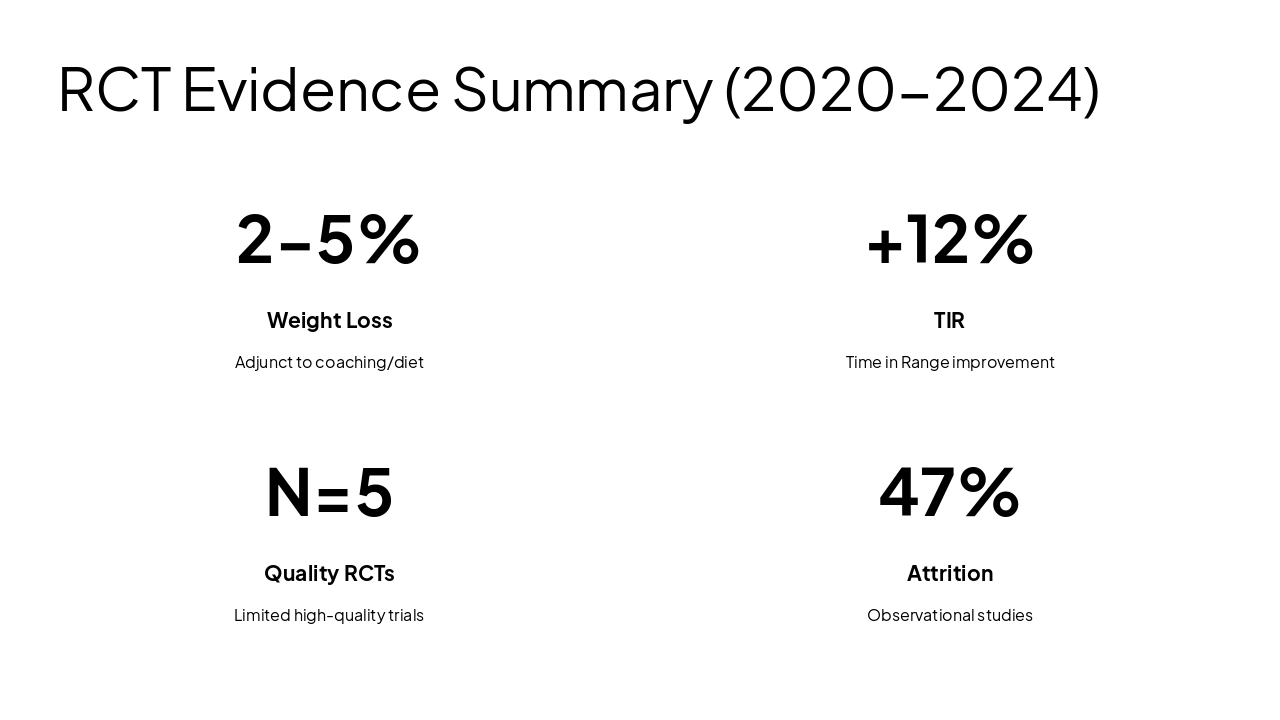
2020–2024 Landscape
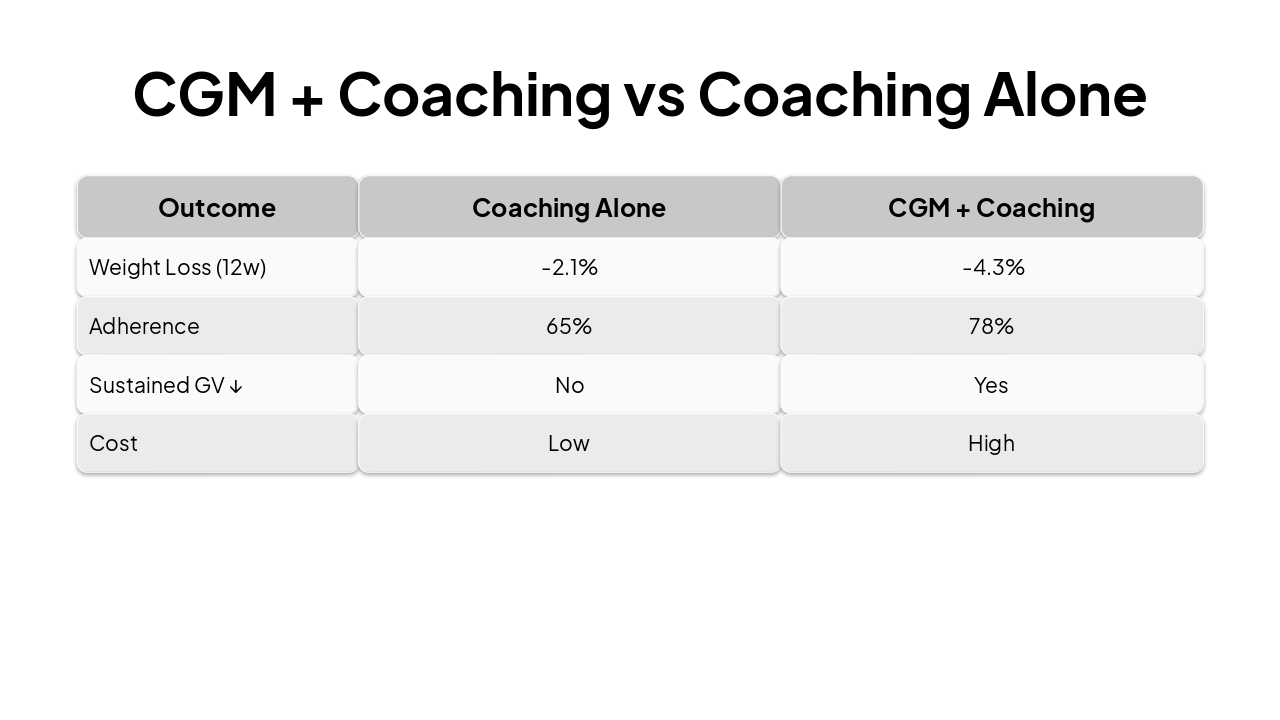
| Outcome | Coaching Alone | CGM + Coaching |
|---|---|---|
| Weight Loss (12w) | -2.1% | -4.3% |
| Adherence | 65% | 78% |
| Sustained GV ↓ | No | Yes |
| Cost | Low | High |
4
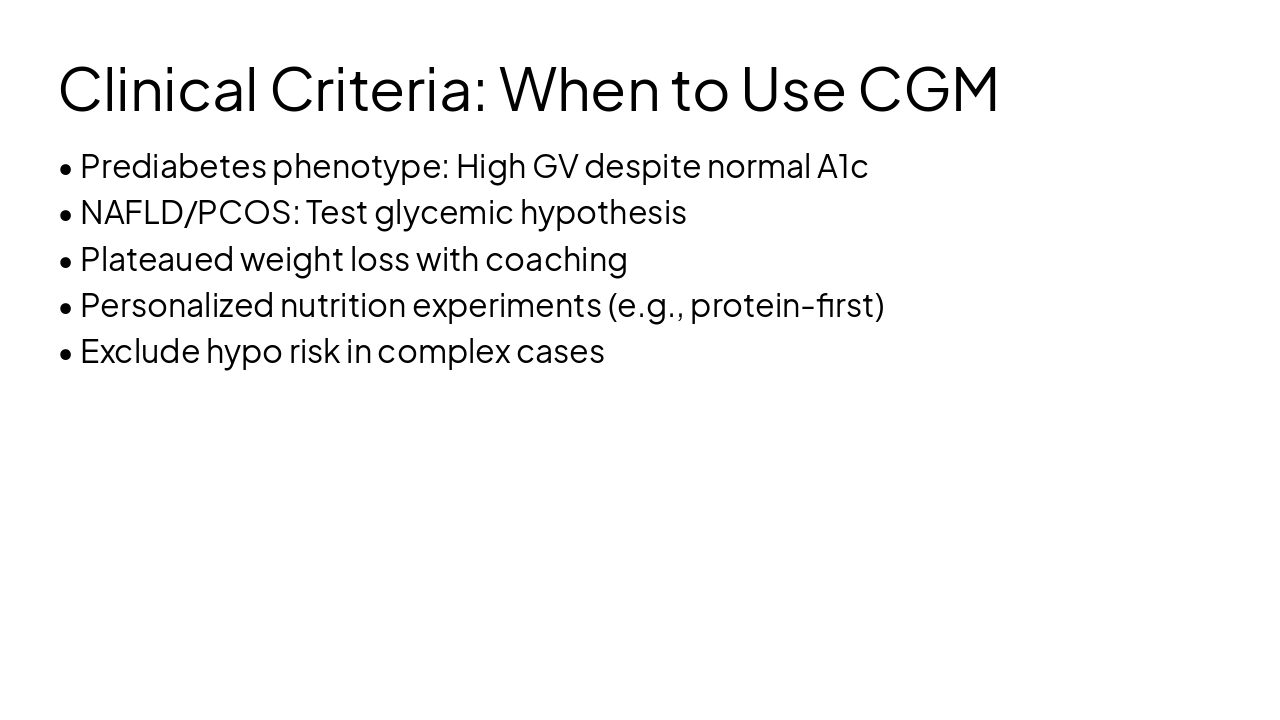
Prediabetes Phenotype & Select Cases
---
Photo by Annie Spratt on Unsplash
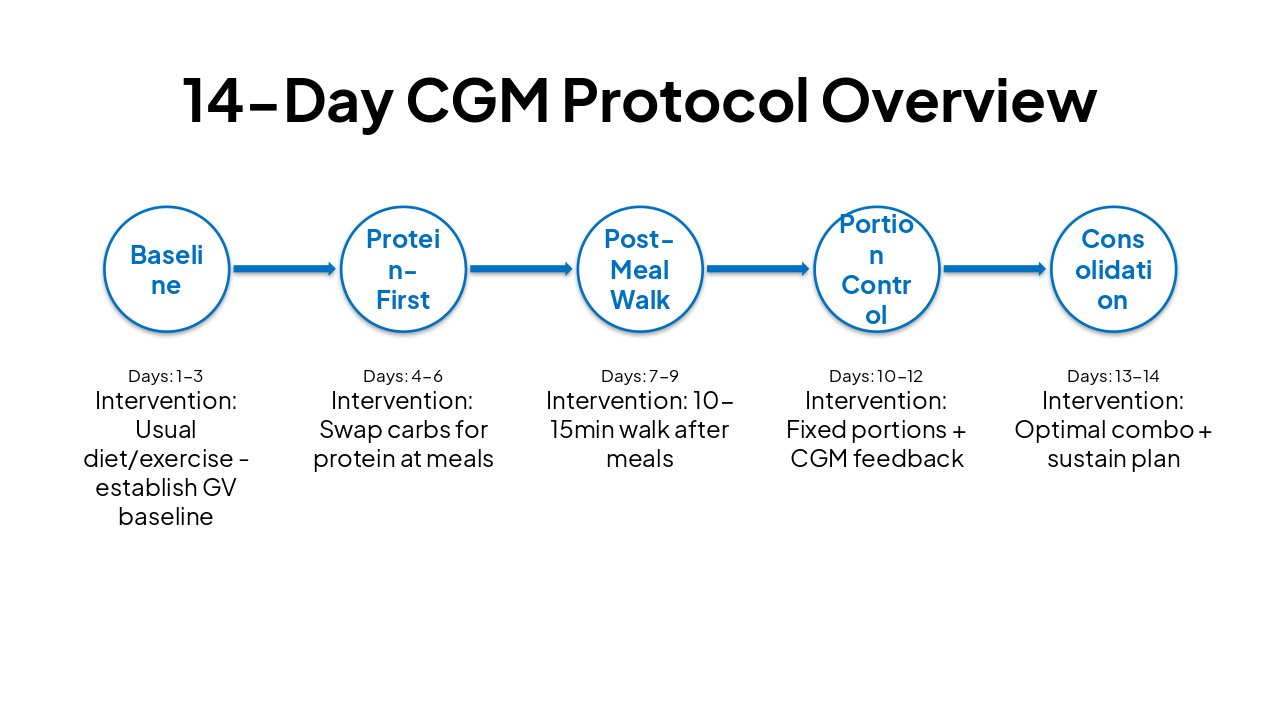
| Phase | Days | Intervention |
|---|---|---|
| Baseline | 1-3 | Usual diet/exercise - establish GV baseline |
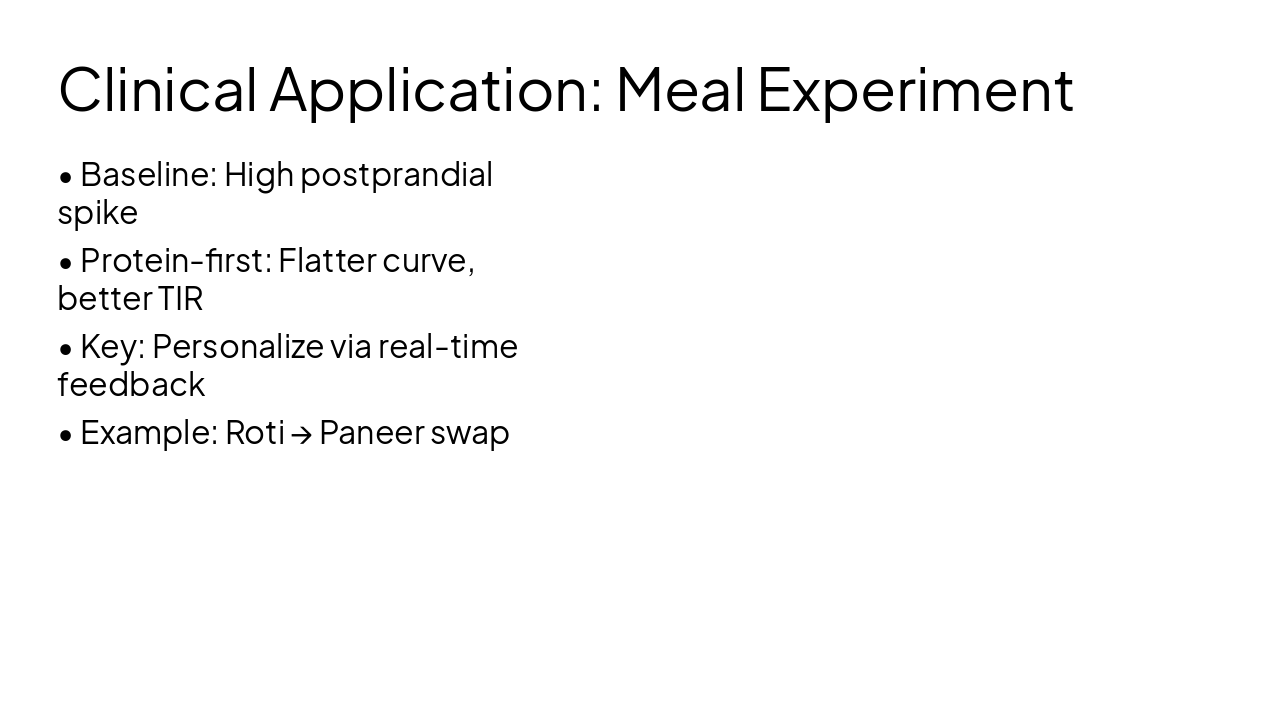
| Protein-First | 4-6 | Swap carbs for protein at meals |
| Post-Meal Walk | 7-9 | 10-15min walk after meals |
| Portion Control | 10-12 | Fixed portions + CGM feedback |
| Consolidation | 13-14 | Optimal combo + sustain plan |
5
Ideal RCT Design
---
Photo by National Cancer Institute on Unsplash

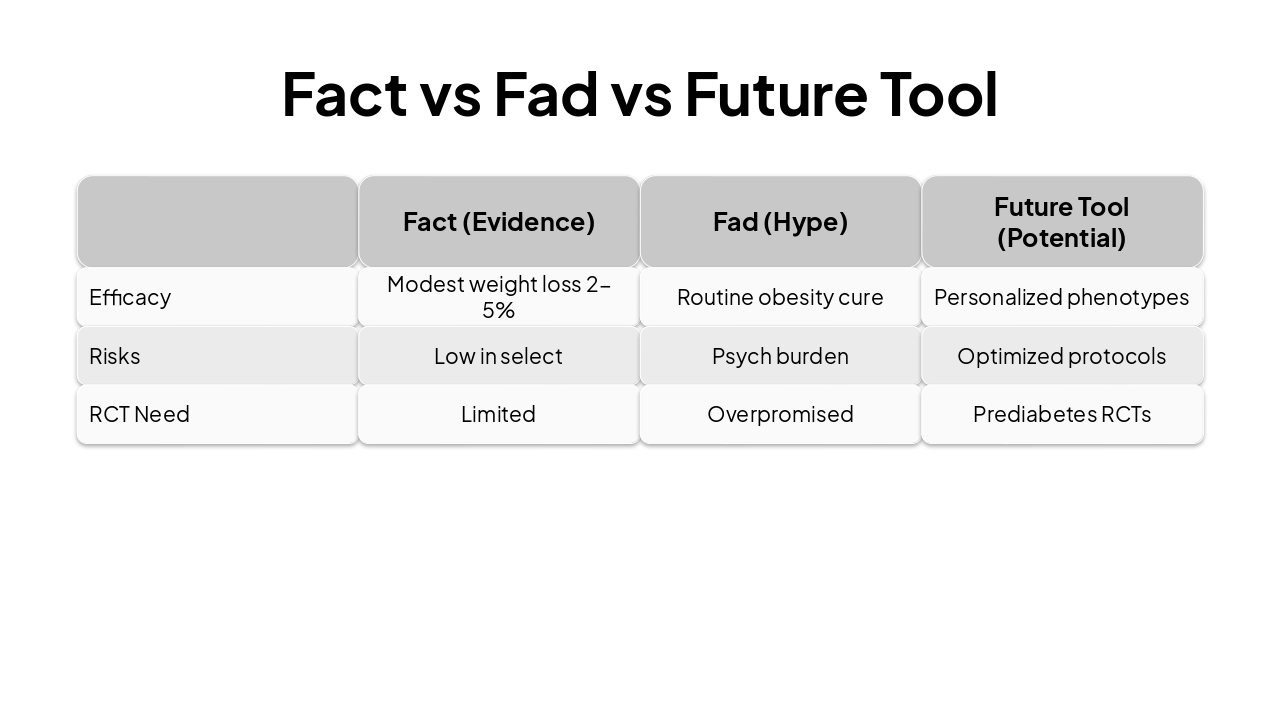
| Fact (Evidence) | Fad (Hype) | Future Tool (Potential) | |
|---|---|---|---|
| Efficacy | Modest weight loss 2-5% | Routine obesity cure | Personalized phenotypes |
| Risks | Low in select | Psych burden | Optimized protocols |
| RCT Need | Limited | Overpromised | Prediabetes RCTs |
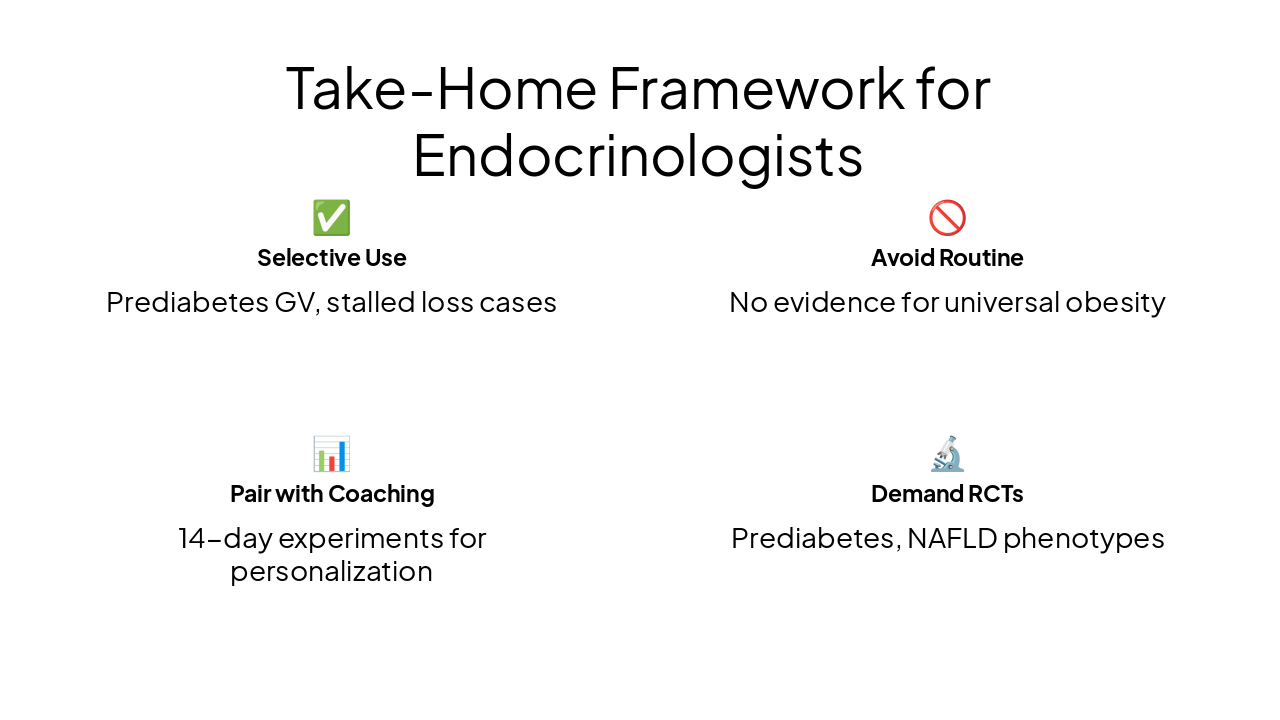
✅ Selective Use Prediabetes GV, stalled loss cases
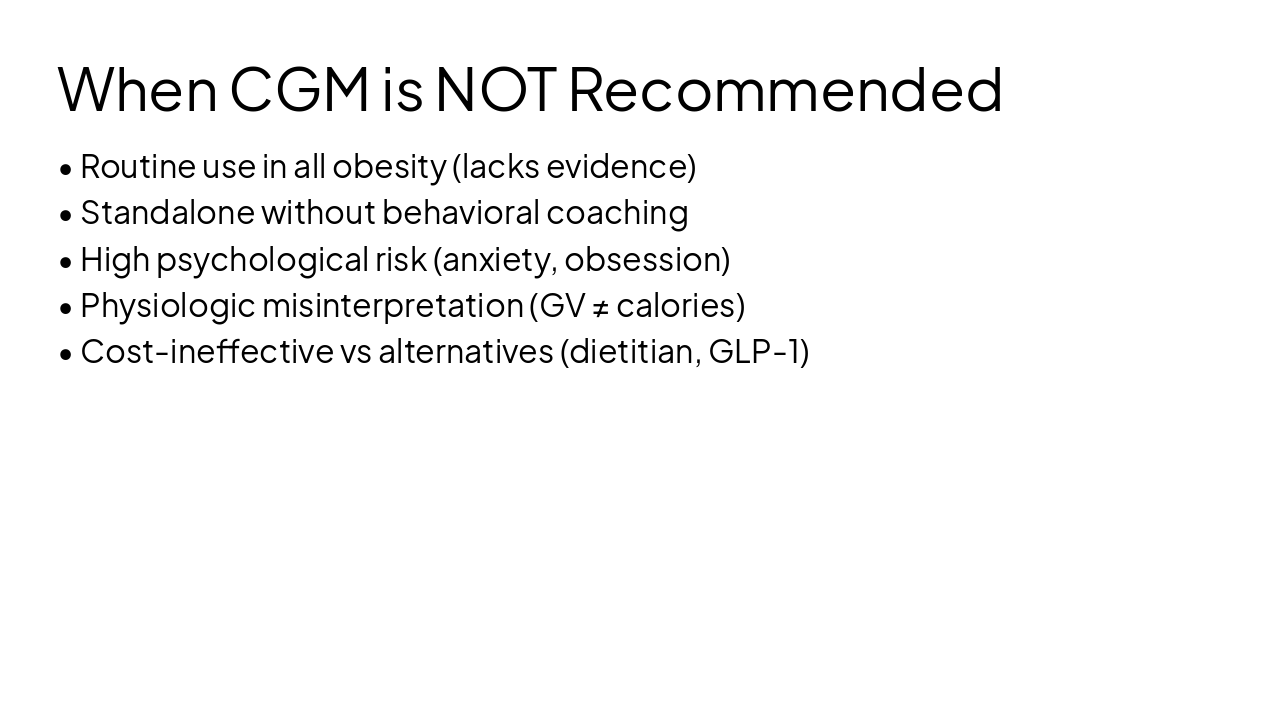
🚫 Avoid Routine No evidence for universal obesity
📊 Pair with Coaching 14-day experiments for personalization
🔬 Demand RCTs Prediabetes, NAFLD phenotypes
CGM in Obesity: Fact for Select Cases Future Tool with RCTs Selective, Not Routine
Questions? Contact for Protocol Details
Explore thousands of AI-generated presentations for inspiration
Generate professional presentations in seconds with Karaf's AI. Customize this presentation or start from scratch.