Slide 1 of 13
Slide 1 - Case Presentation – Adrenal Insufficiency with Urosepsis
Case Presentation: Adrenal Insufficiency with Urosepsis
Intern Doctor, Medicine Unit 6 | Fiza Arman
Generated from prompt:
Redesign this medical case presentation into a clean, modern, highly presentable slide deck. Design requirements: - Light theme: white background with olive green and dark green accents - Clean medical-style typography - Add subtle, cute adrenal gland illustrations as background elements (not distracting) - Improve spacing, hierarchy, and readability Content improvements: - Fix grammar and spelling - Convert dense paragraphs into bullet points - Highlight key clinical findings, vitals, and lab abnormalities - Add clear section headers: Chief Complaints, History of Present Illness, Past History, Examination, Investigations, Diagnosis, Differentials, Management Considerations - Emphasize adrenal insufficiency case relevance - Present lab data in clean tables - Add “Key Takeaways” slide Keep all original medical data but make it concise and visually structured. Title: Case Presentation – Adrenal Insufficiency with Urosepsis Author: Fiza Arman, Intern Doctor, Medicine Unit 6
This medical case presentation outlines a patient with adrenal crisis triggered by urosepsis, including chief complaints, history, vitals, labs, diagnosis, differentials, management, and key clinical takeaways for high suspicion and rapid steroid干预.
Case Presentation: Adrenal Insufficiency with Urosepsis
Intern Doctor, Medicine Unit 6 | Fiza Arman
1
Chief Complaints and History of Present Illness
2
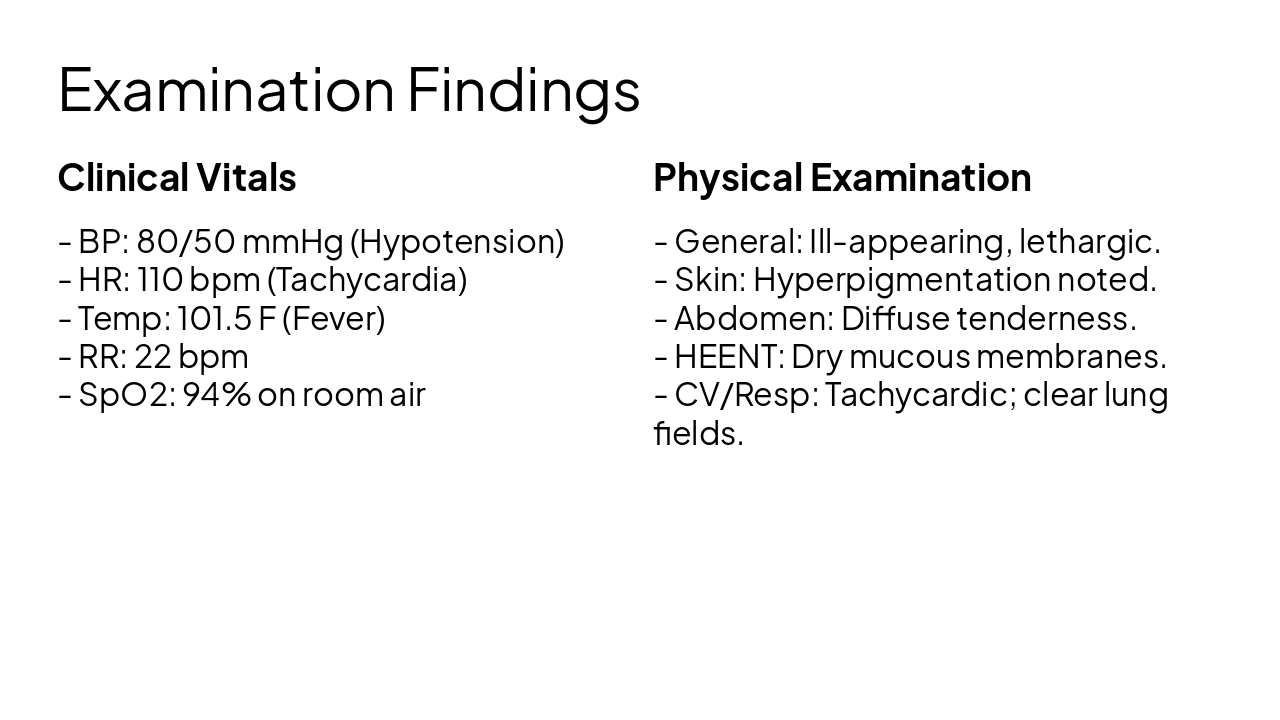
Physical Examination, Vitals, and Medical History
Clinical Vitals
Physical Examination
3
Laboratory findings and clinical reasoning
---
Photo by The Cleveland Museum of Art on Unsplash
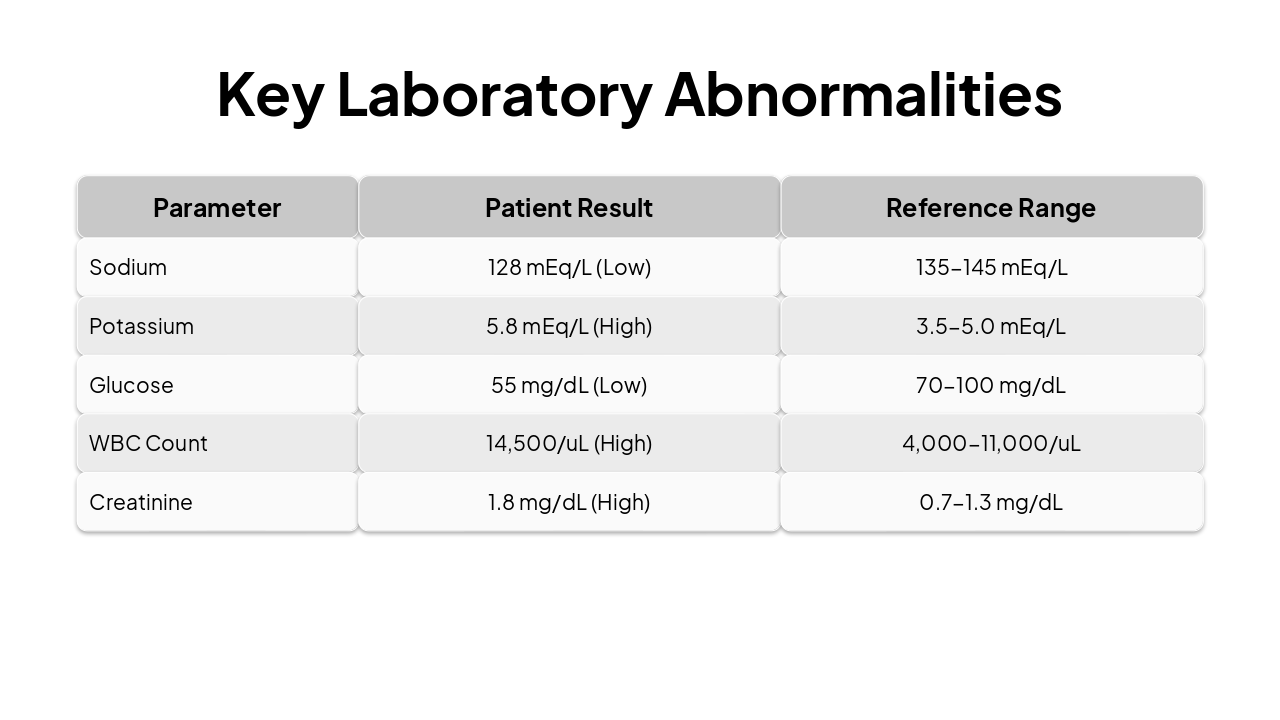
| Parameter | Patient Result | Reference Range |
|---|---|---|
| Sodium | 128 mEq/L (Low) | 135-145 mEq/L |
| Potassium | 5.8 mEq/L (High) | 3.5-5.0 mEq/L |
| Glucose | 55 mg/dL (Low) | 70-100 mg/dL |
| WBC Count | 14,500/uL (High) | 4,000-11,000/uL |
| Creatinine | 1.8 mg/dL (High) | 0.7-1.3 mg/dL |
4
Approach to treatment and key clinical takeaways
Adrenal Insufficiency requires high index of clinical suspicion.
Thank you for your attention. Questions?
Explore thousands of AI-generated presentations for inspiration
Generate professional presentations in seconds with Karaf's AI. Customize this presentation or start from scratch.
