Slide 1 of 13
Slide 1 - Clinical Case Presentation
Autoimmune Pancreatitis vs. Pancreatic Cancer
A Clinical Case Study: Diagnostic Challenges in Differential Diagnosis
---
Photo by Logan Gutierrez on Unsplash
Generated from prompt:
Hi, im a doctor and i have a presentation this sunday, it is a clinical case presentation about auto immune pancreatitis and pancreatic cancer. this is the finished presentation content and information wise, however except for the header, it is ugly, old , the text doesnt pop out, nothing about it is modern or sleek. i want you to transform it into a modern, sleek, classy and smooth presentation. Here are my do and dont: Do not change the first slide, i like it as it is, Do not change any of the information or the content itself, not even a letter, Do not overly design or overly complicate things, i want a smooth experience for the people im presenting to, Lets see what you got!
This clinical case study explores the diagnostic challenges in differentiating autoimmune pancreatitis (AIP) from pancreatic cancer in a 62-year-old male patient with jaundice. It covers clinical history, lab/imaging findings, differential diagnosis,
Autoimmune Pancreatitis vs. Pancreatic Cancer
A Clinical Case Study: Diagnostic Challenges in Differential Diagnosis
---
Photo by Logan Gutierrez on Unsplash
---
Photo by Ayanda Kunene on Unsplash
1
Patient Demographics and Chief Complaints
---
Photo by Immo Wegmann on Unsplash
2
Review of Laboratory Data and Radiological Evidence
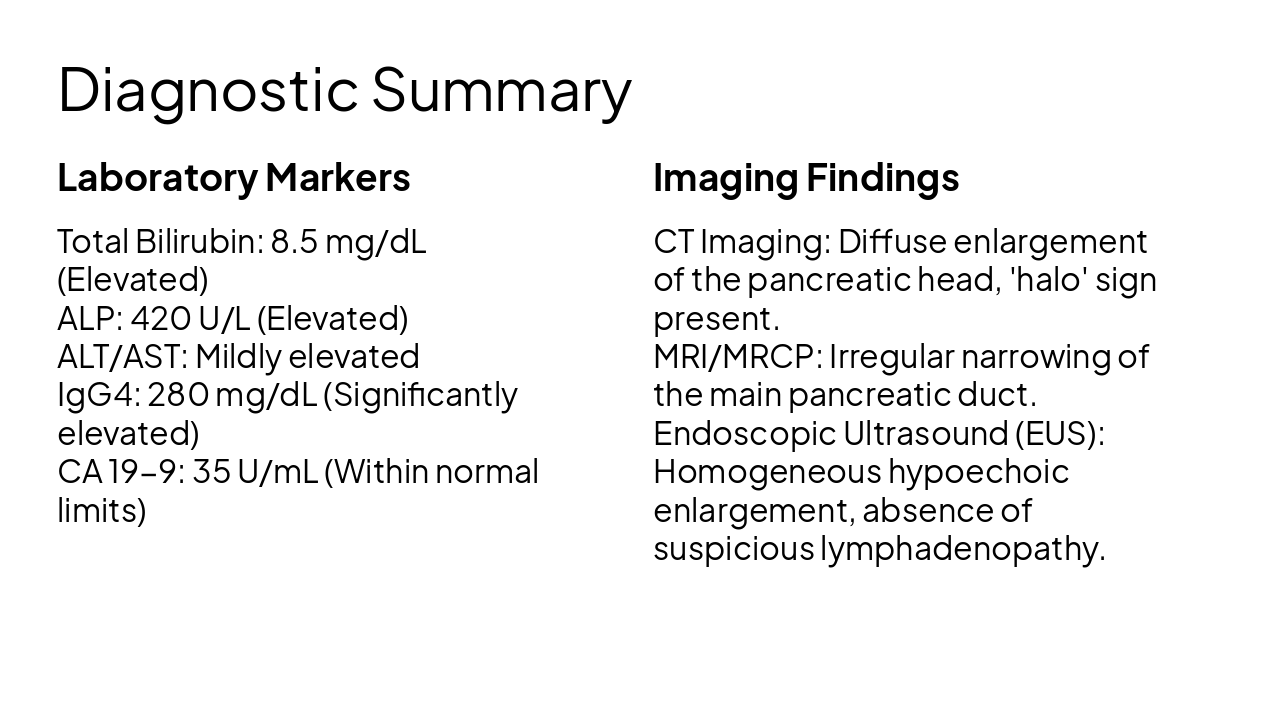
Laboratory Markers Total Bilirubin: 8.5 mg/dL (Elevated) ALP: 420 U/L (Elevated) ALT/AST: Mildly elevated IgG4: 280 mg/dL (Significantly elevated) CA 19-9: 35 U/mL (Within normal limits)
Imaging Findings CT Imaging: Diffuse enlargement of the pancreatic head, 'halo' sign present. MRI/MRCP: Irregular narrowing of the main pancreatic duct. Endoscopic Ultrasound (EUS): Homogeneous hypoechoic enlargement, absence of suspicious lymphadenopathy.
3
Differentiating AIP from Pancreatic Adenocarcinoma
---
Photo by Brett Jordan on Unsplash
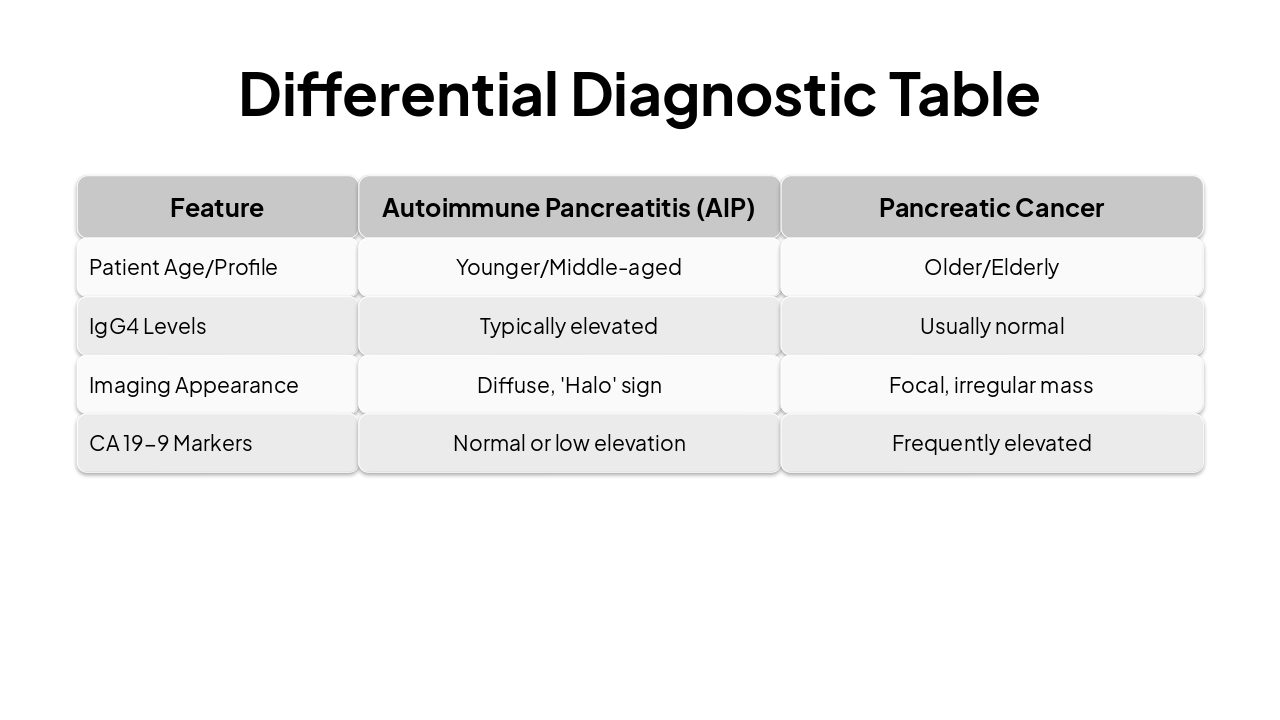
| Feature | Autoimmune Pancreatitis (AIP) | Pancreatic Cancer |
|---|---|---|
| Patient Age/Profile | Younger/Middle-aged | Older/Elderly |
| IgG4 Levels | Typically elevated | Usually normal |
| Imaging Appearance | Diffuse, 'Halo' sign | Focal, irregular mass |
| CA 19-9 Markers | Normal or low elevation | Frequently elevated |
4
Correlation of Clinical Findings and Conclusion
When clinical and radiological evidence are ambiguous, consider autoimmune etiologies like AIP before invasive interventions. Prompt recognition leads to rapid therapeutic response.
Final clinical pearls for the audience
Explore thousands of AI-generated presentations for inspiration
Generate professional presentations in seconds with Karaf's AI. Customize this presentation or start from scratch.
